Due studi recenti sull'utilizzo terapeutico della cannabis in alcune patologie offrono spunti di riflessione interessanti per pazienti e operatori sanitari: da un lato il position statement della Fondazione Gimbe, dall'altro la revisione sistematica sulla rivista Epidemiologia e Prevenzione.
Due studi recenti sull'utilizzo terapeutico della cannabis in alcune patologie offrono spunti di riflessione interessanti per pazienti e operatori sanitari.
La Fondazione Gimbe ha pubblicato in questi giorni un "position statement" Uso terapeutico della cannabis nel dolore cronico: efficacia ed effetti avversi. Diverse le motivazioni che hanno indotto a realizzarlo. Il dolore cronico, dal punto di vista epidemiologico, è fortemente legato a necessità terapeutiche e, di conseguenza, ha effetto sulla produzione di cannabis. Inoltre, i medici saranno sempre più spesso chiamati a discutere di benefici e rischi della cannabis con i loro pazienti.
Nel mese di ottobre anche sulla rivista Epidemiologia e Prevenzione è uscita una revisione sistematica sull’efficacia terapeutica e la sicurezza della cannabis per i pazienti affetti da sclerosi multipla, dolore neuropatico cronico e pazienti oncologici che assumono chemioterapie, realizzata dal Dipartimento di epidemiologia del Servizio sanitario regionale del Lazio.
In entrambi i documenti sono riportate le evidenze della possibile efficacia di questa terapia, che è stata peraltro oggetto di molti altri studi recentemente pubblicati.
L’Associazione Italiana Sclerosi Laterale Amiotrofica (Aisla) avvia un’indagine tramite un questionario per realizzare il primo registro nazionale delle persone affette da Sla.
L’Associazione italiana sclerosi laterale amiotrofica (Aisla) avvia un’indagine per realizzare il primo registro nazionale delle persone affette da Sla.
Ad oggi in Italia non esiste un registro nazionale sulla Sla che raccolga e tenga traccia delle diagnosi e del numero di persone affette dalla malattia. Proprio per questo motivo Aisla ha affidato all’Associazione del registro dei pazienti neuromuscolari il compito di creare il primo registro nazionale sulla Sla con finalità di ricerca e di raccolta di dati clinici e anagrafici.
Al fine di organizzare al meglio il registro, Aisla lancia un questionario per ottenere una prima mappatura, non solo dei già noti centri clinici preposti alla diagnosi della malattia ma, soprattutto, degli ospedali e dei medici che quotidianamente seguono i malati dopo la diagnosi.
Il questionario è disponibile, da oggi fino al 15 febbraio 2018 sul sito Aisla.
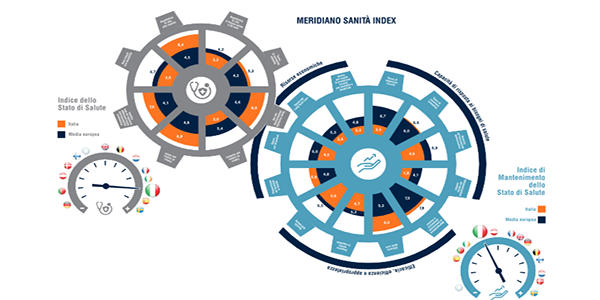
A Roma è stato presentato ieri il XII rapporto Meridiano sanità e Meridiano sanità index. Il rapporto, curato da The European House - Ambrosetti, misura la salute degli italiani e il funzionamento del sistema sanitario del nostro paese. Leggi i principali articoli di commento.
A Roma è stato presentato ieri il XII rapporto Meridiano sanità e Meridiano sanità index. Il rapporto, curato da The European House - Ambrosetti, misura la salute degli italiani e il funzionamento del sistema sanitario del nostro paese. Meridiano Sanità Index offre un'immediata rappresentazione grafica dell'Italia rispetto alla media europea per 8 key performance indicator dello stato di salute e 12 del mantenimento dello stato di salute.
Ecco sintesi e principali commenti al rapporto in alcuni giornali:
Il nuovo Indice di qualità dell’aria appena diffuso dall’Agenzia europea dell’ambiente e dalla Commissione europea, consente agli utenti di controllare la qualità attuale dell’aria nelle città e nelle regioni europee.
Il nuovo Indice di qualità dell’aria, consente agli utenti di controllare la qualità attuale dell’aria nelle città e nelle regioni europee.
Sulla base di misurazioni provenienti da più di 2000 stazioni di monitoraggio presenti in tutta Europa, l’indice è costituito da una mappa interattiva che mostra la situazione della qualità dell’aria locale a livello della stazione, sulla base di cinque inquinanti chiave che nuocciono alla salute delle persone e all’ambiente: il particolato (PM2.5 e PM10), l’ozono troposferico (O3), il diossido di azoto (NO2) e il diossido di zolfo (SO2). L’indice è integrato da nuove schede informative nazionali che forniscono informazioni aggiornate sulla qualità dell’aria per i vari paesi membri, completando la relazione annuale Air Quality in Europe dell’AEA per il 2017, pubblicata a ottobre.
Inoltre il report Urban PM2.5 Atlas: Air Quality in European cities, pubblicato dalla Commissione Europea, mappa specificatamente le origini del particolato fine, come polvere, fumo, fuliggine, polline e particelle di suolo, nelle città dell’UE. Nella relazione viene evidenziata l'importanza di fornire informazioni per migliorare le politiche sulla qualità dell'aria e supportare le autorità nella scelta delle azioni più efficienti.
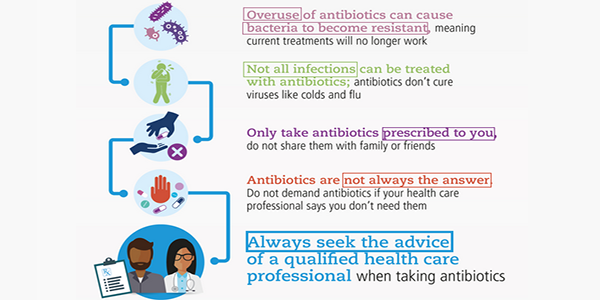
In occasione della settimana mondiale della consapevolezza antibiotica e della giornata europea dedicata allo stesso tema (18 novembre) abbiamo pensato di riunire i materiali informativi che Oms, Ecdc e Ministero della salute hanno presentato.
In occasione della settimana mondiale della consapevolezza antibiotica e della giornata europea dedicata allo stesso tema (18 novembre) il Ministero della salute presenta il nuovo Piano nazionale di contrasto all’antimicrobico-resistenza (PNCAR) 2017-2020.
Il Piano nazionale di contrasto all'antimicrobico-resistenza
Approvato con intesa tra Governo, Regioni e Province autonome di Trento e Bolzano e basato su un approccio intersettoriale, il PNCAR individua strategie coerenti con le indicazioni fornite dall’Oms, nell’ottica dell’approccio one health, “una salute”, per affrontare e contrastare in maniera efficace un fenomeno, che non riguarda solo l’ambito umano, ma interessa da vicino anche il settore veterinario e quello della produzione degli alimenti, senza dimenticare le ripercussioni sull’ambiente.
Il PNCAR è stato predisposto da un gruppo di lavoro multidisciplinare, istituito nel 2015 presso la Direzione generale della prevenzione sanitaria del Ministero della salute (DGPREV), a cui hanno partecipato gli esperti delle altre Direzioni generali, l’Aifa, l’Istituto superiore di sanità, il Laboratorio nazionale di riferimento dell’antibiotico-resistenza e rappresentanti delle Regioni e di alcune Società scientifiche.
Il PNCAR individua 6 ambiti di intervento:
Sorveglianza
Prevenzione e controllo delle infezioni
Uso corretto degli antibiotici - compresa Antimicrobial Stewardship
Formazione
Comunicazione e Informazione
Ricerca e Innovazione
Il Piano declina una serie di azioni a livello delle Istituzioni centrali, regionali e locali, finalizzate a migliorare i livelli di consapevolezza e di informazione/educazione nei professionisti della salute, nei cittadini e negli stakeholders. Si punta anche a monitorare il fenomeno dell’AMR e dell’uso degli antibiotici; migliorare la prevenzione e il controllo delle infezioni, in tutti gli ambiti; ottimizzare l’uso di antimicrobici nel campo della salute umana e animale; aumentare/sostenere ricerca e innovazione. Per guidare e dare piena attuazione al Piano e alla strategia nazionale di contrasto in esso delineata, all’interno della DGPREV del Ministero è stato istituito, con Decreto dirigenziale del 3 novembre 2017, un Gruppo tecnico di coordinamento, monitoraggio e aggiornamento del Piano e della Strategia nazionale di contrasto dell’AMR.
Il PNCAR recepisce inoltre le conclusioni e le raccomandazioni che l'ECDC ha fornito dopo la visita in Italia per valutare la situazione epidemiologica locale, discutere specifiche problematiche e criticità, concordare l'applicazione di opportune strategie migliorative. L’ECDC, infatti, ha anche il mandato di supportare gli Stati Membri nel controllo e prevenzione delle malattie infettive, incluse le infezione da germi antimicrobico-resistenti e, all’interno delle sue attività, ha sviluppato un processo di visite nei paesi europei. La visita in Italia si è svolta dal 9 al 13 gennaio 2017 e, dopo avere visitato 3 regioni - che rispecchiano realtà differenti -, e alcuni ospedali, parlato con esperti e rappresentanti delle istituzioni, i delegati dell’ECDC hanno stilato le loro conclusioni - evidenziando il pericolo rappresentato dall’AMR e la necessità di un coordinamento per affrontare il fenomeno, affinché le buone pratiche già consolidate in alcune aree del Paese divengano patrimonio comune nella pratica quotidiana degli operatori e dei cittadini - e fornito una serie di raccomandazioni, in un documento finale Country Visit Report - ECDC Country visit to Italy to discuss antimicrobial resistance issues.
In linea con i Piani di azione internazionali
La predisposizione del Piano risponde all’esigenza di individuare strategie coerenti con le richieste e le indicazioni fornite dall’Oms, che nel maggio del 2015, nel corso della 68° Assemblea Mondiale della Sanità, ha adottato il Global action plan on antimicrobial resistance (GAP) sollecitando azioni coordinate tra la stessa Oms, la Fao (Food and Agriculture Organization) e l'Oie (World Organisation for Animal Health). All’adozione del GAP hanno fatto seguito, dunque, le Risoluzioni sulla lotta alla resistenza agli antimicrobici adottate nello stesso anno da Fao ed Oie e l'iniziativa della Commissione del Codex Alimentarius relativa alla necessità di riesaminare e aggiornare gli standard, i codici e gli orientamenti connessi alla resistenza agli antimicrobici. Nel settembre del 2016, durante la 71° Sessione dell’Assemblea Generale delle Nazioni Unite, si è svolto un meeting di alto livello sul tema dell’AMR, nel corso del quale è stata approvata una Dichiarazione politica allo scopo di accrescere la consapevolezza dei governi e accelerare l’impegno globale sul problema.
L'antimicrobico-resistenza e il G7
Dal 2015, inoltre, l’AMR è entrata, come tema prioritario nell’Agenda Salute del G7 e dal 2016 in quella del G20. Il 5 ottobre 2017 è stata uno dei temi della riunione dei capi dei servizi veterinari del G7 a Roma e il 5 e 6 novembre 2017 è stata al centro della Riunione dei Ministri della salute del G7 a presidenza italiana che si è tenuto a Milano. Le linee strategiche sono delineate nel comunicato United towards Global Health: common strategies for common challenges.
L'antimicrobico-resistenza in veterinaria
Per dare attuazione alle linee previste dal Piano, in particolare per gli aspetti riguardanti il miglioramento della consapevolezza e della comprensione del fenomeno dell’AMR, la Direzione generale della sanità animale e dei farmaci veterinari (DGSAF), prendendo spunto dalle indicazioni dell’Oie, ha predisposto materiale informativo per l’uso prudente degli antibiotici, rivolto alle Istituzioni, ai medici veterinari, ai distributori, ai produttori di mangimi medicati e alle industrie farmaceutiche e diffuso in occasione della settimana mondiale della consapevolezza antibiotica. La condivisione di conoscenze e di informazioni corrette resta il presupposto essenziale per l’uso consapevole e appropriato degli antimicrobici, elemento che rappresenta il fulcro delle politiche nazionali, europee e internazionali per il contrasto all’AMR.
I dati EARS-Net mostrano che la resistenza antimicrobica rimane una grave minaccia per la salute pubblica in Europa. Per le infezioni batteriche invasive, il trattamento rapido con agenti antimicrobici efficaci è particolarmente importante ed è uno degli interventi più efficaci per ridurre il rischio di un esito fatale. Le elevate percentuali, riportate in molti paesi, di “isolati”con resistenza ai principali gruppi antimicrobici, sono pertanto di grande preoccupazione e costituiscono una grave minaccia per la sicurezza del paziente.
L'uso prudente di antimicrobici e le strategie di prevenzione e controllo delle infezioni in tutti i settori sanitari, rappresentano le pietre miliari di un intervento efficace per prevenire la selezione e la trasmissione di batteri resistenti agli agenti antimicrobici. Nel 2016 la resistenza combinata a diversi gruppi di antibiotici ha continuato ad aumentare per le specie di Escherichia coli e Acinetobacter. Questa situazione è di grande preoccupazione poiché i pazienti infetti con questi batteri resistenti a molteplici farmaci (multidrugresistant) hanno opzioni di trattamento molto limitate.
Le azioni della Commissione Europea e la dichiarazione del 15 novembre 2017
Nel giugno 2017 è stato presentato un nuovo piano d'azione contro la resistenza antimicrobica, sulla base dell'esperienza acquisita in quasi due decenni di azioni dell'UE nei settori della salute umana e della sanità veterinaria, e tenendo conto degli insegnamenti tratti dalle precedenti azioni dell'UE. Il piano d'azione evidenzia la necessità di affrontare la questione dell'uso degli antimicrobici simultaneamente nelle persone e negli animali, tenendo al contempo maggiormente conto del ruolo della resistenza antimicrobica nell'ambiente. Evidenzia altresì che l'UE dovrebbe svolgere un ruolo guida nella lotta alla resistenza antimicrobica e offrire un valore aggiunto alle azioni degli Stati membri.
L'obiettivo del nuovo piano d'azione è mantenere la capacità di curare efficacemente le infezioni negli esseri umani e negli animali. Gli obiettivi principali sono i seguenti: "fare dell'UE una regione in cui si applicano le migliori pratiche", "stimolare la ricerca e l'innovazione" e "definire il programma mondiale".
Il 15 novembre Vytenis Andriukaitis, Commissario per la Salute e la sicurezza alimentare, e Carlos Moedas, Commissario per la Ricerca, la scienza e l'innovazione, hanno rilasciato una dichiarazione che riassume la posizione e le azioni nella lotta all’antibiotico resistenza nella UE.